
Migraine Management for Otolaryngologists
PRACTICAL TREATMENT OF CHRONIC MIGRAINE / SINUS HEADACHE / VESTIBULAR MIGRAINE FOR OTOLARYNGOLOGISTS
A substantial percentage of the dizzy and sinus pressure patients you see in the Otolaryngology clinic actually have symptoms attributable to migraine and will have more improvement with migraine treatment than with any other treatment. Neurologists often do not want to treat these patients as their symptom burden may only be mild to moderate, and they will not meet criteria for either migraine or vestibular migraine. Overall only 16% of migraine sufferers who are treated ever see a neurologist. The remainder bulk of migraine treatment is delivered by primary care. Primary care physicians also have difficulty treating these patients as migraine because they differ so much from classic migraine headache patients. My experience after speaking with dozens of otologists who send identified patients to neurology or to primary care is that they do not know anything about how those patients have fared. Patients will benefit from direct treatment at the Otolaryngology office, and the experience will be as gratifying for you the physician as for your patients.
This outline does not consider treatment of migraine headache which benefits from abortive treatments when sporadic and preventive and abortive therapy when chronic. Offering treatment to patients with migraine is simple medicine.
Chronic migraine is unusually common in the otolaryngology clinic and these patients with frequent symptoms will benefit more from preventive therapy than any other migraine treatment. My treatment protocol is relatively simple. I use four primary drugs: nortriptyline, diltiazem or verapamil, propranolol and topiramate. In some cases of vestibular migraine I will use low dose clonazepam as an adjunct.
The first part of treatment is enrolling patients in the idea that they do have a form of migraine, one that they have never heard of, but that you as a doctor recognize. They need to understand that their symptoms will respond to the same preventive treatments as migraine headache. We are not talking about abortive treatments but preventive treatments. The preventive treatment of migraine has 2 parts: one is reduction of migraine triggers, and the other is elevation of the migraine threshold for triggering of migraine.
Migraine triggers and threshold before and after treatment
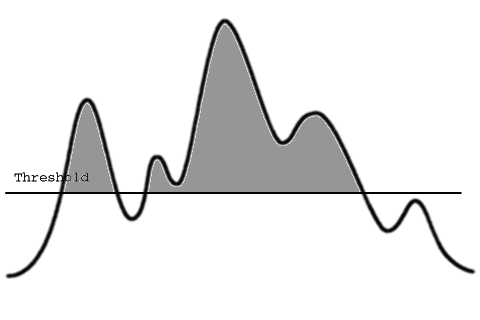
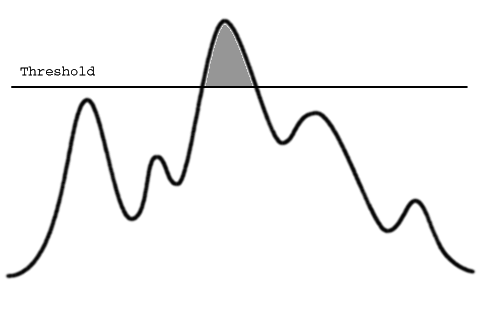
Medications that stabilize the central nervous system are used to elevate the threshold for triggering of migraine. The reduction in triggers is done by eliminating or reducing migraine triggers in the diet as much as possible and by treating any obvious sources of discomfort in the head and neck. I have a large “no list” of food triggers on my web site, and I tell people to try to reduce caffeine and to eliminate other foods present on the list to only once a week. There is also a “yes list” that is more practical to shop with. In addition, if they have a history of seasonal allergies and especially if they have a history of exacerbation of symptoms during seasons I have them do allergy testing. This has become an important part of treatment for some of my patients. I encourage all patients to use diet and medication strategies to get well fast. When they improve they can add back as desired. Some want to avoid medication and we agree to try diet restriction for six weeks first, especially if they are obviously overboard on caffeine, chocolate, red wine, cheeses or other strong triggers. Also, it is useful to let patients know that medications are not forever; they are used to break the cycle of chronic headache and can be removed in most cases. More on this later.
THE MEDICATIONS
Nortriptyline for anyone over 50
For patients over 50 the first “go to” medication is low dose nortriptyline (10 mg capsules, take 2HS Dispense 60 refillx5). Nortriptyline may work as well as it does in these patients because it has so many mechanisms of action: all tricyclic antidepressants are synthesized from an antihistamine base so has some antihistamine action with mild vestibular suppressant activity. It is also a medium potency calcium and sodium channel blocker, as well as an SNRI. In addition, it is anticholinergic; this is important because many chronic migraine sufferers have increased parasympathetic tone as a part of their migraine syndrome that leads to hypotension and orthostasis, as well as GI symptoms. Parasympathetic tone changes also cause tearing, nasal congestion and rhinorrhea.
Nortriptyline is taken before bed; 1HS the first week then 2HS after that. They are usually concerned by two things: one is the side-effect list which is indeed impressive, but I assure patients that the list was made by people who were taking 100-350mg for depression, and that this dose is extremely small in comparison. Patients are also concerned that nortriptyline is an antidepressant and need reassurance that at this low dose causes mood alteration (an improvement) only in a rare patient. Many patients are already taking an SSRI or other antidepressant and I have not had any problems in 20 years with a patient who was taking other antidepressants who then had serotonin syndrome because of taking low-dose nortriptyline. Risks may be higher if patients take psychiatric doses. Occasionally a well meaning pharmacist will raise a red flag to the patient who is taking other serotonin drugs so it is important to let patients hear reassurance from you first. Serotonin syndrome is very rare. I reassure all patients that if they feel badly on any medication they do not need my permission to discontinue it. I do not believe that patients need to tolerate severe medication side effects for months in order to trial a medication.
The response rate to nortriptyline is really high, over 60%, so it is the first go to medication for patients over 50. It can be used in younger patients but many younger patients feel tired on it. Twenty milligrams is the index dose of nortriptyline in this patient group, meaning if they are going to respond it it there will be at least some response at that dose. Almost all patients will notice they sleep better. If they have difficulty waking up in the morning with a slow start for an hour or two, I have them take it an hour or two earlier before going to bed. Once again, if they do not tolerate the medication for any reason I do not insist that they take it, and we move on to the next medication. If they come back and have had a substantial response, maybe 30-50% of symptom reduction, and they are tolerating the medication, then I have them increase to 30 mg a night for 3 weeks and then, if needed, to 40 mg. I see them back in another 6 weeks. Generally, I see these patients every 6 weeks to check their symptoms. I also remind them of and discuss how they are doing with their diet at every visit. Weight gain can be a problem with nortriptyline because of a carbohydrate craving. If patients do gain weight they need to be aware of calories and portion control. Other adverse effects that can be limiting are dry mouth and constipation. There are a few patients for whom nortriptyline works great but for whom constipation is a real issue. I have them take magnesium daily at whatever dose is needed to stay regular. Any form will do but magnesium citrate is the most laxative(250mg daily to 500-BID is the usual range).
Overall about sixty percent of my patients take only 20mg of nortriptyline, twenty percent take 30 or 40 mg, and twenty percent take 50-75 mg. Patients who get to higher doses are those who are compatible with it and seem to tolerate it easily.
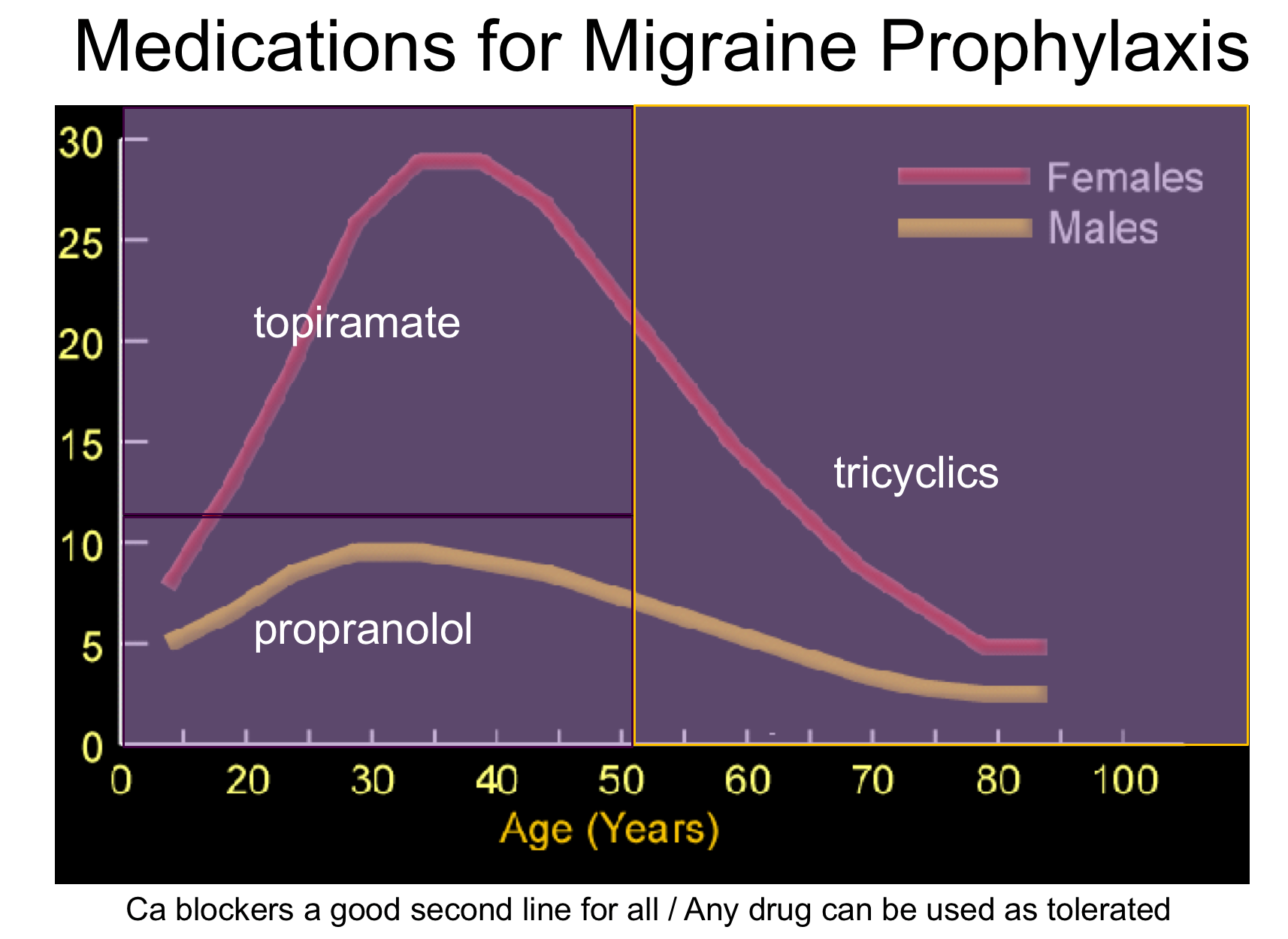
Use topiramate for females under 50.
I give them 25 mg tablets and escalate by 25 mg a week to 50 mg b.i.d.(topiramate 25mg, I HSx1wk, then 1BIDx1wk, then 1am1pmx1wk then 2BID disp120) By tapering up they can avoid most of the side-effects, then we taper up from there if needed. Only 25% of patients need more than 50mg bid. Some patients get up to 100 mg or even 150mg BID. A lot of these patients also have headaches, sometimes not severe but headaches nonetheless, and those disappear on treatment because even though they are mild they are migraine. I remind these patients that they are fortunate their headaches are not “fully flowered”. When prescribing I remind patients that topiramate can cause numbness and tingling in the hands and feet, but that goes away if the same dose is maintained for a few weeks, a taste change and decrease in appetite that often causes modest weight loss, and in 20%, cognitive disturbance. Cognitive problems are the most common reason for discontinuation of therapy. Young women tolerate and accept it because of the prospect of weight loss so I tend to start with topiramate in young women. Trokendi is a new 24 hour version of topiramate that reduces cognitive side effects to only 4% but is not covered by some insurances. It is worth fighting for in patients who respond uniquely to topiramate but have limiting side effects.
The other 2 medications you need to know are the antihypertensives; the beta blocker propranolol and calcium channel blockers diltiazem and verapamil are useful for these patients. Patients will take one or the other and never both: the combination of beta and calcium channel blockade could be dangerous, is almost never used by cardiologists, and is a hard no. If a patient is already on an antihypertensive medication, no problem; additional BP lowering of 10mm Hg can be expected by adding an additional agent.
For men younger than 50 start with Propranolol
I start at 80 mg XR once daily and increase to 120 mg if they have a response that is incomplete. Some take 240mg. Watch for depression and weight gain, and warn athletes that it could limit peak athletic performance. This is usually not an issue unless they are competitive. Uncontrolled asthma is a contraindication as are calcium channel blockers. In my experience Propranolol is the best tolerated and effective medication for young men.
Diltiazem is a good second line agent at all ages
I start with 120 mgXR and consider going up to 240 mgXR if they have a response. Verapamil is cheaper but has inconvenient TID dosing. I usually taper verapamil up by writing 80mg daily for 1 week, then BID for a week, then TID. Calcium channel blockers can cause constipation and weight gain. Magnesium can be helpful.
Patients worry about these drugs if they already have low blood pressure and a lot do because of the increased parasympathetic tone associated with chronic migraine. Fortunately, because their vasculature is already relaxed antihypertensives can exert their desired effects in the CNS without aggravating and even improving hypotension, except in a rare patient. A PCP has never called me upset that I started these meds when the patient is on other blood pressure agents.
Clonazepam is a drug I use as a last resort in Vestibular Migraine and only in patients who have an actual symptom of a rocking sensation or severe anxiety that is a cause or aggravating factor of their problem. I find that patients with rocking respond better to clonazepam than anything else. I prescribe at 0.5 mg twice daily. It is often a good temporary add-on medication for patients whose symptoms are related to a significant life stress as a trigger and who are having difficulty coping. It can serve as a bridge while getting the help of a cognitive behavioral therapist. It is uniquely effective for symptoms of rocking dizziness but is usually prescribed only after trials of other classes of medication have failed because it is a controlled substance. It should be avoided if there is a history of substance abuse. Clonazepam is GABA-ergic and long acting. It has more effect on central vestibular pathways and on otolith function than cholinergic agents like meclizine. I prescribe 0.5mg BID and instruct patients to start with ½ or even ¼ of a tablet BID, the smallest dose necessary to control symptoms. The group of patients who need this medication are quite severely affected and most tolerate 0.5BID with no reduction, and even an improvement, of work performance. I never prescribe higher than 0.5 mg BID; if patients need or want more it is a warning of a possible addictive tendency. Stopping the medication is a taper that halves the dose every 2 weeks until no longer practical. A sudden withdrawal after more than 2 months will generally result in 3-4 days of irritability and sleeplessness; it is uncomfortable but not dangerous.
Finally, I reassure patients that these medications are not forever. They may need them for a year, two or three both now and at future points in their lives. My rule is this: if any patient become asymptomatic for 6 months they should be asking the very reasonable question: ”I wonder if I still need this medication?”. We then attempt to taper every 2 weeks to see if symptoms increase. If not, keep going. Fifty percent of well controlled patients are successful getting off. A quarter find they still need medication but at a lower dose, and a quarter find out right away that they need to continue as before. I often have patients on a maintenance dose attempt a taper prior to a 6 month follow up visit. We discuss the outcome and feel more certain we are on track when we make decisions in the context of the result of a taper attempt. They accept the medication best if they know it is preventing symptoms.
Once you start treating these patients your practice will begin to transform: you will become the only practitioner who is able to find solutions for a lot of patients. Each year attendees from my courses follow up with reports of the gratification they have experienced in applying this knowledge. If you would really like to feel comfortable prescribing all of these medications and would like to see all aspects of migraine management all the way to nerve blocks and Botox, I would suggest you come spend a day or two with me sometime in Wilmington, Delaware. You will see how we choose and exactly how we manage their medications. More importantly you will see lots of patients who are being treated successfully in this way for symptoms which may be receiving other care in your home practice.
There is a lot of information on my web site that may be helpful: simply google Teixido and Patient Information or go to: https://www.entad.org/for-patients/patient-information-dr-teixido/. It has the diagrams and materials I show my patients, and the diet lists. All patients are emailed this link to my web site material as homework: https://www.entad.org/for-patients/patient-information-dr-teixido/migraine-more-than-a-headache/ Take a minute to look at it if you can.
Information Provided by Dr. Michael Teixido, MD
Dr. Teixido is a board certified Otolaryngologist and Otologist/Neurotologist, with a special interest in medical and surgical conditions that affect hearing and balance. He is actively pursuing his goals of advancing the study and understanding of problems involving hearing and balance as a result of hereditary hearing conditions in his own family. View Dr. Teixido's Full Bio
FOULKSTONE
PLAZA
1401 Foulk Road.,
Suite 205
Wilmington, DE 19803
Phone: (302) 998-0300
Fax: (302) 478-8069
Greenville
Location
1011 Centre Rd,
Suite 200,
Wilmington DE 19805
Phone: (302) 998-0300
Fax: (302) 543-8456
MIDDLETOWN
CROSSING
306 East
Main Street
Middletown, DE 19709
Phone: (302) 998-0300
Fax: (302) 376-5251
NEWARK- IRON HILL
CORPORATE CENTER
700 Prides Crossing
Suite 200
Newark, DE 19713
Phone: (302) 998-0300
Fax: (302) 998-5111