
Meniere’s Disease
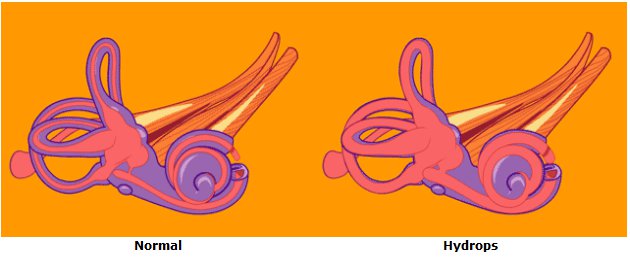
Endolymphatic hydrops and Meniere’s disease are disorders of the inner ear. Although the cause is unknown, it probably results from an abnormality of the fluids of the inner ear. In most cases, only one ear is involved but both ears may be affected in up to 20% of patients.
THE SYMPTOMS
A patient with endolymphatic hydrops may experience any combination of the below described symptoms:
Vertigo is the most troublesome symptoms of endolymphatic hydrops. The vertigo of endolymphatic hydrops may occur in attacks of a spinning sensation which may result in nausea and sometimes vomiting. The vertigo may last for as short as a few minutes or as long as hours. During attacks the patient is usually unable to perform activities normal to their work and home life. Sleepiness may follow for several hours and an off-balance sensation may last for days following an attack. Some patients do not have attacks of spinning vertigo but have episodes of disequilibrium in which their head may feel as if it is swimming or the floor seems to be shifting beneath their feet.
There may be an intermittent hearing loss during the disease, especially in the low pitches, but a fixed hearing loss involving tones of all pitches commonly develops in time. It is not uncommon for loud sounds to be very uncomfortable and to appear distorted in the affected ear.
The excessive fluid pressure on the hearing nerves may also cause tinnitus. The tinnitus of endolymphatic hydrops may sound like crickets or a high tone but most commonly sounds like a low pitched hiss which may increase and decrease in intensity as the fluid pressure increases and decreases.
The increased fluid pressure in the inner ear may also result in a sensation of fullness or pressure within the ear which cannot be cleared by popping the ear.
The symptoms of endolymphatic hydrops may be only a minor nuisance or can become disabling especially if the attacks of vertigo are severe, frequent, and occur without warning. In patients who have all of the above described symptoms, we apply the term Meniere’s disease after the French otologist Prosper Meniere who first described this inner ear syndrome in 1856
Watch an animation depicting the fluctuating symptoms of Meniere’s disease.
HOW IS A DIAGNOSIS OF ENDOLYMPHATIC HYDROPS MADE?
The diagnosis of Meniere’s disease is usually made by identifying the cardinal symptoms of ear fullness, fluctuating hearing loss, episodic vertigo and characteristic roaring or seashell tinnitus. In addition to a history and physical examination you will be asked to undergo some diagnostic studies to rule-out causes for your symptoms other than an inner ear disorder. This may take the form of blood tests, hearing tests, x-rays, CT scans or MRI scans of the brain and inner ear or electrocochleography.
Perhaps the most important testing for any patient with Meniere’s disease is serial audiometry. An audiometric examination (hearing test) is performed to look for characteristic types of hearing loss in the affected ear. Because the hearing can change from day to day in patients with Meniere’s disease, audiograms on sequential visits are obtained to look for signs of fluctuating hearing levels that are characteristic of Meniere’s disease. Speech discrimination (the ability to distinguish between words like “sit” and “fit”) is often diminished in the affected ear and is also tested for. Tympanometry is also performed in order to determine if pressure symptoms could be originating from the middle ear rather than the inner ear.
Electrocochleography may indicate increased inner ear fluid pressure in some cases of endolymphatic hydrops. In this test a tiny electrode is placed in the ear canal near the inner ear. The tiny electrical impulses from the hair cells of hearing in the inner ear are then recorded and characteristic changes which are seen in conditions of inner ear pressure are looked for.
An ENG ( electronystagmography) and VEMP (vestibular evoked myogenic potentials) exam may be performed. Just as the hearing test measures the function of the hearing nerve endings, the ENG and VEMP measure the strength and function of the nerve endings in the balance end of the inner ear. With time, the balance function in an ear with Meniere’s disease will decrease and the intensity of vertigo will decrease. The ENG is done in a darkened room. Recording electrodes are placed near the ears. Wires from the electrodes are attached to a machine similar to a heart monitor. Warm and cool water are gently introduced into each ear canal. Since the eyes and ears work in a coordinated manner through the nervous system, measurement of eye movements can be used to test the balance system. In about 50% of patients the balance function is reduced in the affected ear. Other balance tests such as rotational testing or balance platform tests may also be performed to evaluate the balance system.
Computed Tomography (CT scanning) or magnetic resonance imaging (MRI) may be needed to rule out other causes of some of the symptoms the patient is experiencing before they can be attributed to endolymphatic hydrops.
HOW CAN MENIERE’S DISEASE BE TREATED?
The cause of Meniere’s disease is still unknown. Recent research suggests disorders of maintenance of the ion balance in the inner ear fluids may be the root cause of the ear symptoms in Meniere’s disease. The inner ear in patients with Meniere’s disease is often ill because of an outside aggravating factor, such as allergy, typical or atypical migraine, temporomandibular joint or neck problems. If the cause of the irritation to the inner ear can be identified in a patient, avoiding and treating that cause are often more fruitful than concentrating on the ear symptoms themselves. Treatments may involve medication, extensive diet changes, lifestyle changes, introduction of drugs to the inner ear, and surgery.
In patients with no identifiable cause for their Meniere’s disease, a low salt diet and diuretic (water pill) may reduce the frequency and severity of symptoms. In order to receive the full benefit of the diuretic it is important that you restrict your intake of salt to less than 1500milligrams/day and take the medication regularly as directed. Please buy a nutrition handbook that can help you learn which foods we commonly eat that are loaded with salt. Not all foods that are loaded with salt taste salty!
If you are experiencing prominent balance symptoms from your endolymphatic hydrops, antivertigo medications such as Antivert (generic name: Meclizine) or Valium (generic name: Diazepam) may be prescribed to provide temporary relief during episodes of disequilibrium. If balance symptoms are prominent in your case, you will learn to adjust your medication to the degree of symptoms caused by the swelling of your ears at any particular time. The use of these medications is generally not a good long-term strategy but can allow you to continue to function while more effective treatments are explored.
Fludrocortisone is an effective medication for many patients with Ménière’s disease. It has long been known that the inner ear responds well to sugar steroids called glucocorticoids, but they are not a workable long term medication because of long term steroid side effects. Many ears with Meniere’s disease respond to a mineral steroid, fludrocortisone, which is well tolerated in patients with normal blood pressure, kidney and cardiac function. Fludrocortisone helps the inner ear so much that patients do better even though the medication causes them to retain salt.
MENIERE’S DISEASE AND MIGRAINE
There is increasing interest among ENT physicians in the connection between migraine and Meniere’s disease. While the prevalence of migraine in the US population is 13%, the prevalence of migraine in patients with Meniere’s disease is 56%, and the prevalence of migraine in patients with bilateral Meniere’s disease is 85%.
We have recently discovered that the tiny blood vessels in the inner ear are innervated by branches of the same nerve that innervates the intracranial blood vessels severely affected in migraine attacks. Electrical stimulation of this trigeminal nerve has caused fluid changes in the inner ear which could affect it severely enough to cause a problem like Meniere’s disease. Many patients with migraine and Meniere’s disease who are treated effectively for migraine have experienced an improvement in their Meniere’s symptoms.
<
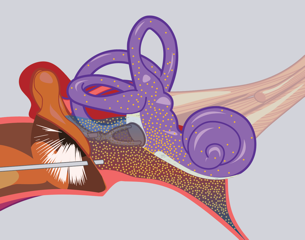
This animation shows blood flow changes and the extravasation of inflammatory substances usually associated with migraine occurring in the inner ear. Changes in the membranous labyrinth also occur. There is increasing evidence to support this migraine mechanism of Menieres disease.
For more information about migraine.
INNER EAR PERFUSION WITH STEROIDS
In most patients, the activity in the affected ear responds well to steroids taken orally. Oral steroids, however, provide only temporary relief and have other physiologic consequences that make them unacceptable for long term treatment. Success in controlling symptoms has been achieved by introducing high doses of steroids directly to the inner ear. This procedure, called Dexamethasone Perfusion avoids the systemic effects of oral steroids. The procedure is simple and safe. The eardrum is viewed under the operating microscope and small spots are numbed with anesthetic applied with a tiny Q-tip. The middle ear is then filled with a solution of steroid in a way that it will contact the membranes of the inner ear. This treatment may give decreased symptoms for months or years and can be repeated easily because the patient can go directly to work on the same day as their perfusion.
Inner ear Perfusion. This illustration shows medication filled into the middle ear diffusing into the labyrinth.
SURGERY FOR ENDOLYMPHATIC HYDROPS
Surgery can be used to control debilitating balance symptoms for endolymphatic hydrops if they cannot be controlled with medications, treatment of underlying causes, or injected steroids. Four types of operations for the control of severe vertigo symptoms are commonly used.
The Endolymphatic Sac Decompression procedure is an outpatient ear operation that preserves hearing. Attacks of vertigo are controlled in three quarters of patients but control is not permanent in all cases. In this operation the inner ear is approached through an incision behind the ear. A small portion of the inner ear (the endolymphatic sac) that protrudes into the bone behind the ear is uncovered and a small drain placed to relieve in the inner ear. Recovery time after this procedure is short compared to other procedures. While hearing is not recovered, most patients experience an improvement in the frequency, intensity and duration of vertigo episodes as well as a decrease in fullness in the operated ear. Endolymphatic sac surgery is selected by patients who wish to solve their vertigo problem but are hesitant to consider procedures which harm inner ear function as a strategy (Gentamycin Perfusion, Labyrinthectomy) unless all other treatments have failed. There is some wisdom in this as Ménière’s disease can develop in the opposite ear in 15 to 20% of patients.

Endolymphatic Sac Surgery. This illustration shows the endolymphatic sac. A silastic drain has been placed into it.
Endolymphatic Duct Occlusion surgery is a technically feasible enhancement of the endolymphatic sac decompression procedure which increases the vertigo response rate to 90%. As in conventional sac surgery the endolymphatic sac is identified but it is then followed behind the inner ear to a point of narrowing that allows for the application of clips to completely obstruct it. While hearing levels do not improve, word clarity scores have risen markedly in many patients. This procedure was developed in Canada, is performed in my practice, and at very few practices in the US or elsewhere.

Endolymphatic Duct Occlusion. A titanium clip is placed across the endolymphatic duct.
Vestibular neurectomy is a procedure in which the balance nerve from the affected inner ear is cut as it courses from the inner ear to the brain. Vertigo attacks are permanently cured in 95% of cases and hearing is preserved in most cases. This is a neurosurgical procedure and is infrequently used since the introduction of gentamycin perfusion of the inner ear (see below) since similar results with decreased risk are possible.
Labyrinthectomy is a procedure which is recommended for those individuals who have no residual hearing in the affected ear. In this operation the inner ear is removed through an incision behind the ear. This results in a 95% rate of control of vertigo attacks. Recovery may take three to six weeks depending on the age of the patient and the demands of their occupation.
INNER EAR PERFUSION WITH GENTAMYCIN
Injections of the antibiotic Gentamicin through the eardrum (Gentamycin Perfusion) can be done in the office to weaken the balance nerve endings in the inner ear so that they cannot cause such severe attacks of vertigo. This medication is much more toxic to the balance nerve endings than the hearing nerves so it can be used in patients with good hearing with acceptable risk. This procedure offers good control of vertigo without any of the risk of general anesthesia or the expense of hospitalization. A weeks long recovery period is typical during which the patient will perform exercises designed to teach the brain to function with one weak labyrinth.
Most patients find that their attacks after gentamycin perfusion are milder and easily managed without impairing their ability to function at their work or inconvenience them. If the attacks are still too strong, a second perfusion can be given, with milder recovery. In our clinic 80% of patients find a single perfusion adequate. Gentamycin perfusion is also referred to as Chemical Labyrinthectomy.
Other operations or treatments may be advised in particular cases. If surgical treatment is necessary, the risks and benefits of surgery will be thoroughly discussed with you. There is no surgical treatment to improve hearing loss or tinnitus associated with endolymphatic hydrops.
Information Provided by Dr. Michael Teixido, MD
Dr. Teixido is a board certified Otolaryngologist and Otologist/Neurotologist, with a special interest in medical and surgical conditions that affect hearing and balance. He is actively pursuing his goals of advancing the study and understanding of problems involving hearing and balance as a result of hereditary hearing conditions in his own family. View Dr. Teixido's Full Bio
FOULKSTONE
PLAZA
1401 Foulk Road.,
Suite 205
Wilmington, DE 19803
Phone: (302) 998-0300
Fax: (302) 478-8069
Greenville
Location
1011 Centre Rd,
Suite 200,
Wilmington DE 19805
Phone: (302) 998-0300
Fax: (302) 543-8456
MIDDLETOWN
CROSSING
306 EastMain Street
Middletown, DE 19709
Phone: (302) 998-0300
Fax: (302) 376-5251
NEWARK- IRON HILL
CORPORATE CENTER
700 Prides Crossing
Suite 200
Newark, DE 19713
Phone: (302) 998-0300
Fax: (302) 998-5111