
Acoustic Neuroma
An acoustic neuroma is a benign tumor which arises from the nerves behind the inner ear and which may affect hearing and balance. The incidence of symptomatic acoustic neuroma is estimated to be between 1 in 75,000 and 1 in 100,000 persons per year. The name acoustic neuroma is a misnomer. The tumor actually arises from the balance nerves which innervate the inner ear in a small bony canal behind the inner ear called the internal auditory canal and should properly be called a vestibular neuroma. The misnomer arises from the fact that the most common presenting complaint for a patient with an acoustic neuroma is a drop in hearing in only one ear which cannot be explained by a one-sided noise exposure or any other ear history. Often the clarity of the sound in the ear is affected out of proportion to the amount of actual hearing loss measured on the hearing test. These tumors are sporadic and there is no known environmental risk factor that makes them occur. There is a small group of patients with a genetic tendency to grow acoustic neuromas. These patients are rare, get tumors on both sides and other intracranial tumors as well and will not be discussed here. There are numerous treatment options for patients with acoustic neuroma and the selection of the best treatment option for a patient is a highly individualized process.
PRESENTING SIGNS AND SYMPTOMS OF AN ACOUSTIC NEUROMA:
As mentioned the most common presenting complaint of a patient with an acoustic neuroma is progressive unilateral hearing loss. Approximately 10% (3-15% in published studies) of patients with acoustic neuroma present with a sudden hearing loss in the effected ear. Patients with sudden hearing loss from an acoustic neuroma experience instantaneous partial or complete loss of hearing. Hearing loss may begin when the tumor is small but some tumors grow to medium size with no hearing loss. Tinnitus is often present along with hearing loss but is rarely the complaint that takes the patient to the doctor and there is no specific character of tinnitus associated with acoustic neuroma. Dizziness is present transiently in approximately 25% of patient’s but may be mild and not result in a visit to the doctor. Headache is extremely uncommon as a presenting symptom of small acoustic neuromas but may be present in the frontal or occipital regions, or over the entire head in half of patients with large tumors (over 30mm). We find that most patients who have headaches on the side of their tumor have a long headache history that likely precede the onset of the tumor growth and which is aggravated by the tumor.
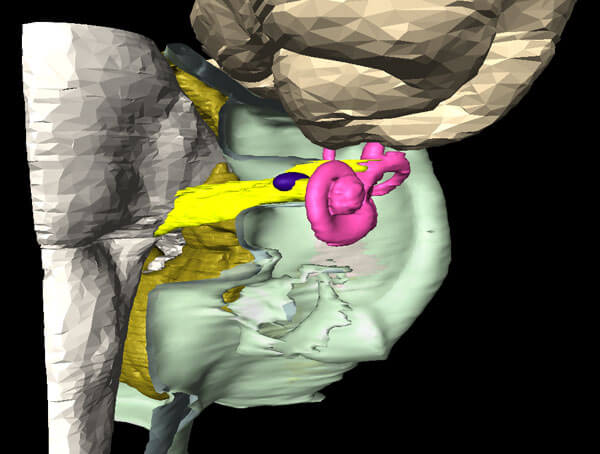
Tiny Acoustic Neuroma: This illustration shows a tiny acoustic neuroma(BLUE) within the internal auditory canal which carries the hearing, balance and facial nerves(YELLOW). Such small tumors may be incidental and it is reasonable to wait for tumor growth or progression of hearing loss before treatment.
THE NATURE AND GROWTH OF ACOUSTIC NEUROMAS:
An acoustic neuroma grows from the insulation cells on the vestibular (balance) nerves. These insulation cells (Schwann cells) generally start growing in a tiny bony canal through which the nerves pass in their course from the brain stem to the backside of the inner ear. The tumor gradually decreases the function of the balance nerves and as it presses on the nerves of hearing, the clarity of hearing and ability of the hearing nerves to transmit nerve impulses of sound will diminish. With time, the tumor will grow from just a few millimeters in size to fill the tiny bony internal auditory canal. It cannot expand easily through the internal auditory canal into the inner ear, so it tends to grow out into the space between the bony canal and the brain stem. This area is called the cerebellopontine angle (CPA) and this is the reason acoustic neuromas are considered a type of cerebellopontine angle tumor.
These benign tumors generally grow 1 to 3 mm per year. One of ten tumors may grow 10 mm in a single year. By the time the tumor reaches 20 mm, it is usually contacting the brain stem and the hearing, balance and facial nerves are stretched over the surface of the slowly growing mass. The contact of the tumor with the brain stem does not represent any immediate danger. If left untreated, the tumor may grow to enormous size (45-75mm) before compressing the brain stem so much that the function of the cerebellum is affected or the circulation of spinal fluid within the brain is blocked and an acute crisis is precipitated. The time which may elapse from the start of growth of an acoustic neuroma to the time of such a crisis may be as long as 20 years. Acoustic neuromas are benign tumors. This means that they do not spread to other parts of the body. They do, however, have serious consequences because of the direct effects they have on the nerves which they compress. Although the facial nerve also runs through the internal auditory canal, with the vestibular nerves and the nerve of hearing, it is unusually resilient and uncommon for patients with small or medium sized tumors less than 25mm to have facial weakness or twitching that leads to the discovery of their tumor.
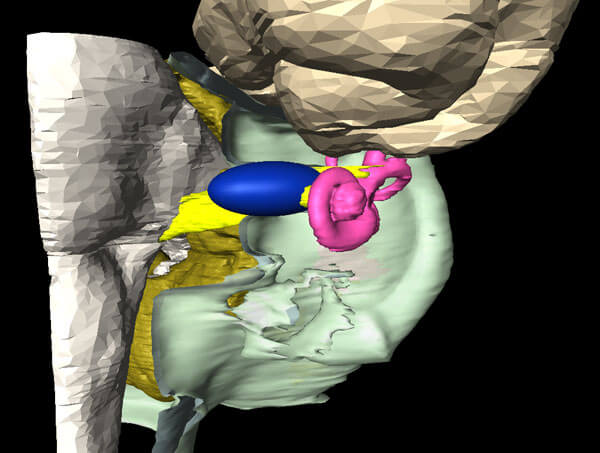
Small Acoustic Neuroma: This neuroma fills the internal auditory canal and is protruding into the space between the bone and the brainstem. It is still far from the brainstem(WHITE) and cerebellum(GOLD). Excellent treatment results can be expected from both radiation and microsurgery in experienced hands.
THE TREATMENT OF ACOUSTIC NEUROMAS:
Patients who been diagnosed with an acoustic neuroma rarely need emergent treatment. Treatment recommendations may involve observation alone, microsurgical excision using one of three surgical approaches or focused radiation using single dose or multidose techniques.
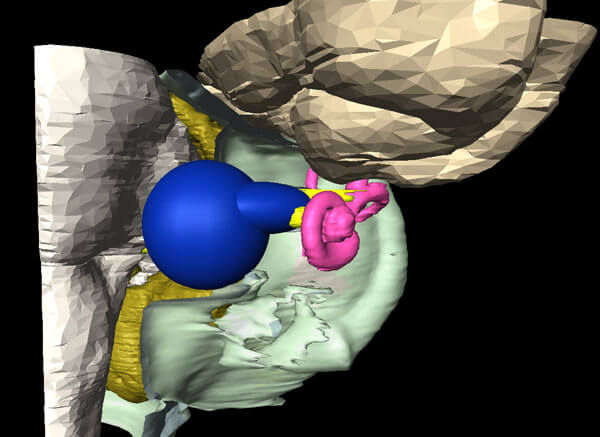
Medium Acoustic Neuroma: At 17 millimeters this tumor just contacts the brainstem. Good results can be expected.
OBSERVATION OF ACOUSTIC NEUROMA:
In patients with small tumors who are over 65 years of age or who have other significant medical conditions, an acoustic neuroma may never be expected to reach such a large size that dangerous consequences from brain compression might result. In these individuals, it is appropriate to simply watch tumor growth understanding that there may be a small chance of a precipitous decline in the patient’s status in later years of life which may require an emergent surgery to reduce the size of the tumor. One well controlled Scandinavian study followed tumors less than 10 mm in size in all individuals aged 65 and over. Only 7% of these individuals ever required emergent surgery later in life and this surgery was often successful at eliminating their symptoms. This would therefore seem to be a reasonable risk for many patients especially if there is a significant chance based on their medical, personal and family histories that heart disease, cancer or other conditions will ultimately be their cause of death. When a decision is made to observe an acoustic neuroma, the tumor is generally observed with repeat MRI scans. There is no known health risk to repeat MRI scanning of brain. This is generally done at yearly intervals but after five years of observation that confirms very slow tumor growth, scanning every other year may be recommended. Observing these tumors rather than treating them may allow a senior patient to avoid the physiologic stress of a surgical procedure or immediate consequences to the facial nerve and hearing that can result from surgery or radiation. Hearing will invariably be lost by the time the tumor reaches a large size but facial nerve function will generally be preserved.
It is rare to find a tumor over 10 mm that does not continue to grow. Very small tumors however, which are still in the internal auditory canal can sometimes be observed yearly and may not grow for five, six or seven years. Autopsy studies show that up to 1% of persons have small acoustic neuromas of which they are not aware. We do not seem to find medium or large tumors in autopsy studies suggesting that some percentage of small tumors may cease to grow and can be considered incidental. It is because of the existence of this group of “incidental” tumors that initial observation may reasonably be recommended for any patient with a tumor less than 10 mm in size, especially if it is asymptomatic and discovered on a scan done investigating another problem.
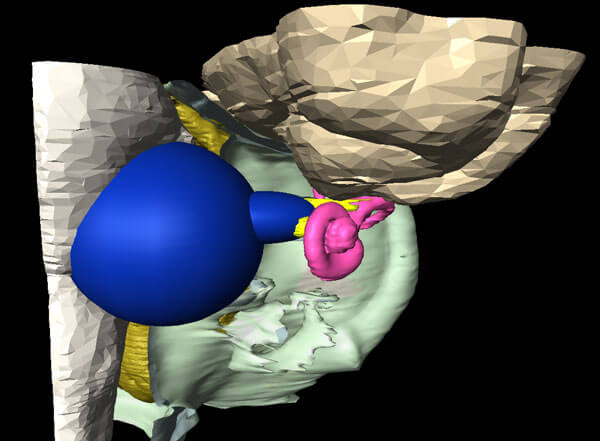
Large Acoustic Neuroma: Tumors over 2.5 centimeters (this one is 2.6 cm) become impacted into the brainstem and cerebellum. Complications associated with surgery and radiation are higher. It is difficult to deliver an adequate dose of radiation to control tumor growth without excessive dosing to the brainstem in tumors larger than this.
SURGICAL REMOVAL OF ACOUSTIC NEUROMAS:
Microsurgical removal of an acoustic neuroma is often recommended for young patients with an acoustic neuroma of any size when tumor growth is proven by enlargement of the tumor on succeeding scans or progression of symptoms like hearing loss attributable to the neuroma. Microsurgical excision involves a collaborative effort between a Neurotologist (an Otolaryngologist with special training in neurology and neurosurgery of hearing and balance disorders) and a Neurosurgeon. Together and with the use of intraoperative nerve monitoring acoustic neuromas can safely be completely excised with minimized risk to the facial nerve, and patient. Preservation of hearing is possible in patients with small tumors only 35% of the time when the cochlear nerve fibers may be preserved. This is because successful hearing preservation also requires successful preservation of the tiny blood vessel to the inner ear. Because this artery is so tiny, delicate and uniformly associated with the capsule of the tumor, its preservation is not always feasible.
Beyond patient safety, preservation of the facial nerve is of paramount importance to acoustic neuroma surgeons and patients. The ability to preserve normal or near normal facial function with tumors up to 15mm is excellent at over 90%. Medium sized tumors 15-25mm may have normal or near normal function after surgery 60% of the time. Results are worse for large tumors. Overall there is a general trend to better results because surgeons have recognized in the 80’s and 90’s that surgical trauma to the nerve can be minimized by leaving small amounts of tumor adherent to the nerve and that these tumor residuals usually do not grow. If growth does occur, years later, their growth can generally be stopped with focused radiation that avoids the risks of re-operating in a scarred operative field.
In addition to the operating team, electrophysiologic monitoring of the facial nerve and all other nerves associated with the tumor is gives immediate feedback to the surgeons that nerves may be suffering irritation or injury during dissection.
The three surgical approaches utilized are a retrosigmoid craniotomy, a translabyrinthine craniotomy and a middle fossa craniotomy. The surgical approach to an individual acoustic neuroma varies depending on the patients hearing status, the size of the tumor and the position of the tumor within the internal auditory canal. With any surgical procedure, there is a small risk of wound infection, postoperative leakage of spinal fluid through the wound, meningitis and stroke. Although these risks are small, they increase with increasing tumor size. Depending on the surgical experience of different surgical teams, different approaches may be recommended for an individual tumor. Surgery usually involves an overnight stay in the Intensive Care Unit and a 3-4 day postoperative hospital stay.
In general, a retrosigmoid craniotomy or middle fossa craniotomy is recommended in patients who have functional hearing where an attempt to preserve hearing is being made. The middle fossa approach is best suited for small tumors still in the internal auditory canal and the retrosigmoid approach is better suited for large tumors which fill the cerebellopontine angle. If the patient already has severely compromised hearing, has a large tumor in which hearing preservation is unlikely or has a small tumor so deeply impacted into the end of the internal auditory canal that hearing preservation is improbable, a translabyrinthine craniotomy which approaches the tumor through the inner ear itself may be recommended. During surgery small pieces of tumor may be left behind on the facial nerve if they cannot be removed without risk of injury to the nerve. These residual pieces of tumor can be followed with MRI scanning but rarely grow because their blood supply has been interrupted.
RADIATION TREATMENT OF ACOUSTIC NEUROMAS:
Radiation treatment for acoustic neuromas is relatively new. The term radiosurgery has been employed because the radiation treatments have been effective enough to replace surgery and can be directed very precisely to the site of the tumor. Radiosurgical techniques differ from traditional radiation therapy in that they focus radiation beams coming from hundreds of directions onto the site of the tumor and the tumor is the only site which receives a critical dose of radiation. This spares the surrounding tissues and the skin which was so commonly burned at the site of entry in traditional radiation therapy. Many different machines have been developed for precise dose delivery. The first of these was called Gamma-Knife radiosurgery. Radiation can also be delivered using the X-Knife or Cyber-Knife. Initial treatment results using these modalities have been very good showing at least 80% prevention of tumor growth. Hearing preservation varies depending on whether a high dose single treatment technique or a low dose multiple treatment technique is utilized. The highest hearing preservation rates currently reported come from multiple treatment (“multiple fraction”) techniques. The reason multiple treatments tend to work better is that the normal tissues like the cochlear nerve surrounding the tumor has a chance to heal and recover in between treatments. Tumor tissue does not have healing ability so the injury accumulates over many days. Treating the tumor all at once is like trying to get a suntan in one long day at the beach instead of with smaller daily exposures over a 10-day period. In one intense exposure, a tan will eventually result but the burn injury to the skin cannot be avoided. Single fraction techniques are still used for patients who have no residual hearing or for whom travel to the treatment center many times is extremely inconvenient because of distance or other factors. Patients after radiation therapy continue to be monitored for tumor growth. There are risks of brain swelling, hearing loss, facial paralysis or post-radiation dizziness with radiation just as in surgery, but these effects tend to developed 5-6 months after the treatment rather than immediately as with surgery. The risk of complications with radiation therapy tends to be slightly lower than with surgery. Surgery may be still be required in up to 20% of patients treated with radiation because of continued tumor growth since radiation cannot be used a second time. Surgery on these irradiated patients tends to be more difficult so patients may not expect the same nerve preservation rates as non-irradiated tumors.
I hope reading this material will have helped you to become better acquainted with the nature of your acoustic neuroma and treatment options available to you. It will enhance your ability to participate in the decision making in your case. There are many other more complex and sometimes rare situations which occur in the treatment of acoustic neuromas which your clinicians will bring up to you if they are relevant in your case.
- Leonard JR, Talbot ML; Asymptomatic Acoustic Neurolemmoma. Arch Otolaryngol 91:117-124, 1970
- Stewart TJ. et al; Occult Schwannomas of the Vestibular Nerve. Arch Otolaryngology 101:91-95, 1975
- Tos M, Thomsen J; Epidemiology of Acoustic Neuromas. J Laryngol Otol 98:685-692, 1985
- Lanser MJ, Sussman SA, Frazer K; Epidemiology, Pathogenesis and Genetics of Acoustic Neuroma. Otol Clinics of N Am 25:499-520, 1992
- Al Sanosi A, Fagan PA, Biggs ND; Conservative management of acoustic neuroma. Skull Base 16:95-100, 2006.
- Chopra R, Kondziolka D, Niranjan A, Lunsford LD, Flickinger JC; Long-term follow-up of acoustic schwannoma radiosurgery with marginal tumor doses of 12 to 13 Gy. Int J Radiat Oncol Biol Phys 68:845-851, 2007.
- Hoistad DL, Melnik G, Mamikoglu B, Battista R, O’Connor CA, Wiet RJ; Update on conservative management of acoustic neuroma. Otol Neurotol 22:682-685, 2001.
- Radu A, Pica A, Villemure JG, Maire R; Indications and results of stereotactic radiosurgery with LINAC for the treatment of acoustic neuromas: preliminary results. Ann Otolaryngol Chir Cervicofac 124:110-114, 2007.
- Silverstein H, McDaniel A, Norrell H, Wazen J; Conservative managemen of acoustic neuroma in the elderly patient. Laryngoscope 95:766-770, 1985.
- Smouha EE, Yoo M, Mohr K, Davis RP; Conservative management of acoustic neuroma: a meta-analysis and proposed treatment algorithm. Laryngoscope 115:450-454, 2005.
Information Provided by Dr. Michael Teixido, MD
Dr. Teixido is a board certified Otolaryngologist and Otologist/Neurotologist, with a special interest in medical and surgical conditions that affect hearing and balance. He is actively pursuing his goals of advancing the study and understanding of problems involving hearing and balance as a result of hereditary hearing conditions in his own family. View Dr. Teixido's Full Bio
FOULKSTONE
PLAZA
1401 Foulk Road.,
Suite 205
Wilmington, DE 19803
Phone: (302) 998-0300
Fax: (302) 478-8069
Greenville
Location
1011 Centre Rd,
Suite 200,
Wilmington DE 19805
Phone: (302) 998-0300
Fax: (302) 543-8456
MIDDLETOWN
CROSSING
306 EastMain Street
Middletown, DE 19709
Phone: (302) 998-0300
Fax: (302) 376-5251
NEWARK- IRON HILL
CORPORATE CENTER
700 Prides Crossing
Suite 200
Newark, DE 19713
Phone: (302) 998-0300
Fax: (302) 998-5111